I got tired of writing about ivermectin as a miracle cure for COVID-19, just as I got tired of writing about hydroxychloroquine as a miracle cure for 2020. As high quality evidence accumulated that hydroxychloroquine doesn't work, it faded in importance and was no longer the preferred wonder drug among conspiracy theorists. Ivermectin became the new hydroxychloroquine when it rose to replace it.
I keep wondering what the new ivermectin will look like, as high quality evidence shows that ivermectin doesn't work. As the evidence from RCTs show it not to be any better than placebo, as well as negative RCTs accumulate and serious deficiencies and probable fraud invalidating the positive RCTs, advocates are increasingly citing lower quality observational studies. It reminds me of a topic that we have been writing about for a long time, and I think that ivermectin is the same thing as COVID-19.
The reason is that ivermectin advocates are back and they are flogging two more studies as proof that ivermectin is cheap.
Here’s another PEER REVIEWED and published study showing 70% reduction in mortality compared to taking Remdesivir. https://t.co/2ppjE4Q5zb
— Kim Iversen (@KimIversenShow) March 8, 2022
I will get to those studies soon. One of the largest antivaccine and medical conspiracy theory websites out there right now is on TrialSiteNews, which is promoting legislative efforts to ignore science and professional recommendations.
The New Hampshire’s state House approved a bill making ivermectin available by a medical prescribers’ “standing order,” meaning pharmacists will be able to dispense the medication without individual prescriptions.
Narrowly approved
The Republican dominated House in Concord voted 183-159 to approve the bill.
Republicans had argued that the drug is already over the counter in several countries and had been used specifically for COVID-19.
According to the legislation, a pharmacist would be able to fill a request for the drug under a “standing order”.
The libertarian think tank, the Brownstone Institute, was founded by Jeffery Tucker.
The New Hampshire House of Representatives has voted to make Ivermectin available at any pharmacy that wants to distribute this drug even without a prescription. It will likely pass the Senate and become law.
It’s a hugely positive breakthrough for medical and pharmaceutical freedom. It’s only tragic that this was not the situation two years ago. The doctors the world over who have rallied behind this treatment believe that many lives might have been saved. If one state in the Northeast had at least made the option available, outcomes might have been very different.
The Epoch Times reports that “Similar bills are pending legislative approval in Oklahoma, Missouri, Indiana, Arizona, and Alaska.”
Magnificent! What’s key here is the concept of human choice.
The irony is very bitter: the vaccine mandates have been universal and people have lost careers for refusing or been rejected for participation in public life. People were forced to get shots of doubtful efficacy in most cases that many people did not want or because they did not see the need and feared their side effects.
Meanwhile, a drug they would have chosen to take was denied to them, again by force, and physicians who believed they were saving lives had their licenses taken away for using their professional discretion.
For a good part of last year, many people in the world could freely buy Ivermectin, a generic drug that at least 8 quality studies have shown to be an effective treatment for Covid-19. It has long been part of the alternative treatment protocol for Covid since it was first tried in early 2020, but never recommended by the FDA, CDC, or NIH. At some point, the CDC was tweeting denunciations of it, somehow with the implication that this treatment was distracting from the main push of vaccine fanaticism.
I quote Mr. Tucker because it's important to remind you that the promotion of ivermectin has become part of the COVID-19 disinformation machine. One of the things that long readers are aware of is how people should be allowed to choose their quackery.
It is important to look at the whole conspiratorial package behind resistance to masks and antivaccine pseudoscience. Tucker makes this case for me. He mocked a CDC cartoon about how to identify health misinformation.
You are welcome to peruse the entire document, the main message of which is that the government is always correct, always knows the most science at the time, while front-line doctors with experience are very likely quacks, crazies, or ruthless profiteers.
Sometimes it seems like the people who produce such propaganda are forever attempting to live in the world of the movie Contagion, where every alternative treatment is a scam promoted by a corrupt “blogger” and where the CDC knows all. This cartoon is a smear in every way.
I looked at the document. It is quite reasonable and mild. It warns people to look out for websites that feature quote-mined quotes, cherry-picked statistics, and old images being recirculated as though they were recent. There are several types of misinformation creators and spreaders, such as the disinformer, the casual sharer, the believer, and others. I wonder why Tucker thinks the CDC is a good place to fact check claims against. I don't.
Tucker pivots to cry "Freedumb!".
This battle is much larger than the legal status of Ivermectin. That’s just one symbol. What’s really at stake here is the idea of medical freedom itself. And freedom is a precondition for scientific inquiry and the search for the truth. It is also essential for public health. This is one of many lessons of the disastrously botched pandemic.
The decisions of the New Hampshire legislature to enshrine that freedom into law in this one instance represent a mighty tribute to the principle and a repudiation of the use of force in disease management.
I realize that ivermectin doesn't work and vaccines don't, but I also know that denialists like him might portray what they are doing as a lie.
On to ivermectin. Again.
One principle that should help you to identify when a medical claim is probably nonsense is that you should look at the quality of evidence cited by the proponents of that medical claim. That's why I mentioned it. We have pointed out how higher quality evidence from randomized controlled clinical trials of acupuncture that use proper blinding and better controls can be found here. Steve Novella pointed out that such studies are nothing more than unblinded trials. Unblinded studies can be justified as hypothesis-generating studies early in the process of investigating a new treatment, but they are not considered the final word. In order to test whether larger randomized studies are justified, nonrandomized observational studies can be justified.
The purpose of the studies is different than what they are called. They aren't so much hypothesis generating as testing. The reason is that pragmatic trials have a specific use in medicine. They are designed to test the real world efficacy of an intervention outside of the control of RCTs. The assumption is that the medical treatment being tested has already been proven to be effective in RCTs and that the pragmatic trial is going to see how much less effective the treatment is when it is released into the wild.
The situation with ivermectin is not the same as before. All the high quality RCTs for ivermectin to treat COVID-19 have been resoundingly negative thus far, and the positive RCTs are the same as the ivermectin advocates prefer lower quality clinical evidence. If the studies are left out, the ivermectin advocates will promote more negative meta-analyses. All higher quality RCTs were tested to see if ivermectin are, as was the case of the higher quality RCTs of acupuncture. There is a definite rule of thumb for the two. The study is more likely to be negative if it is higher quality.
The similarity is that, just as ivermectin advocates cite low quality unblinded studies that might have been acceptable early in the process of investigation, they now cite lower quality studies that aren't RCTs.
Let's take a look at the two studies that Ms. Iverson mentioned. I will remind you of them by citing the Tweets again.
Here’s another PEER REVIEWED and published study showing 70% reduction in mortality compared to taking Remdesivir. https://t.co/2ppjE4Q5zb
— Kim Iversen (@KimIversenShow) March 8, 2022
The Cureus study is entitled Ivermectin Prophylaxis Used for COVID-19: A Citywide, Prospective, Observational Study of 223,128 Subjects Using Propensity Score Matching. Pierre Kory, MD of Front Line COVID-19 Critical Care Alliance, is from Brazil and is one of the investigators. I'm not sure why it's making the rounds now, but it was first published two months ago. I never noticed that it was making the rounds since then. I think part of the reason is that it started out as a preprint. The FLCCC was flogging it in January.
Results of the world’s largest study of ivermectin in COVID have just been posted. Meticulously collected data from hundreds of thousands of patients find massive reductions in hospitalization & death. “Controversy” over. Join us tomorrow for discussion with study investigators https://t.co/BQt9fia44I
— Pierre Kory, MD MPA (@PierreKory) January 5, 2022
You might recall that the FLCCC is a group of doctors who are not at all, but they are spreaders of misinformation. They were caught selling ivermectin and hydroxychloroquine prescriptions to anyone who had the cash.
What about the study itself? You can see how it would impress someone like Ms. Iverson. One notes right away that this study is not a randomized controlled clinical trial, but rather an observational study.
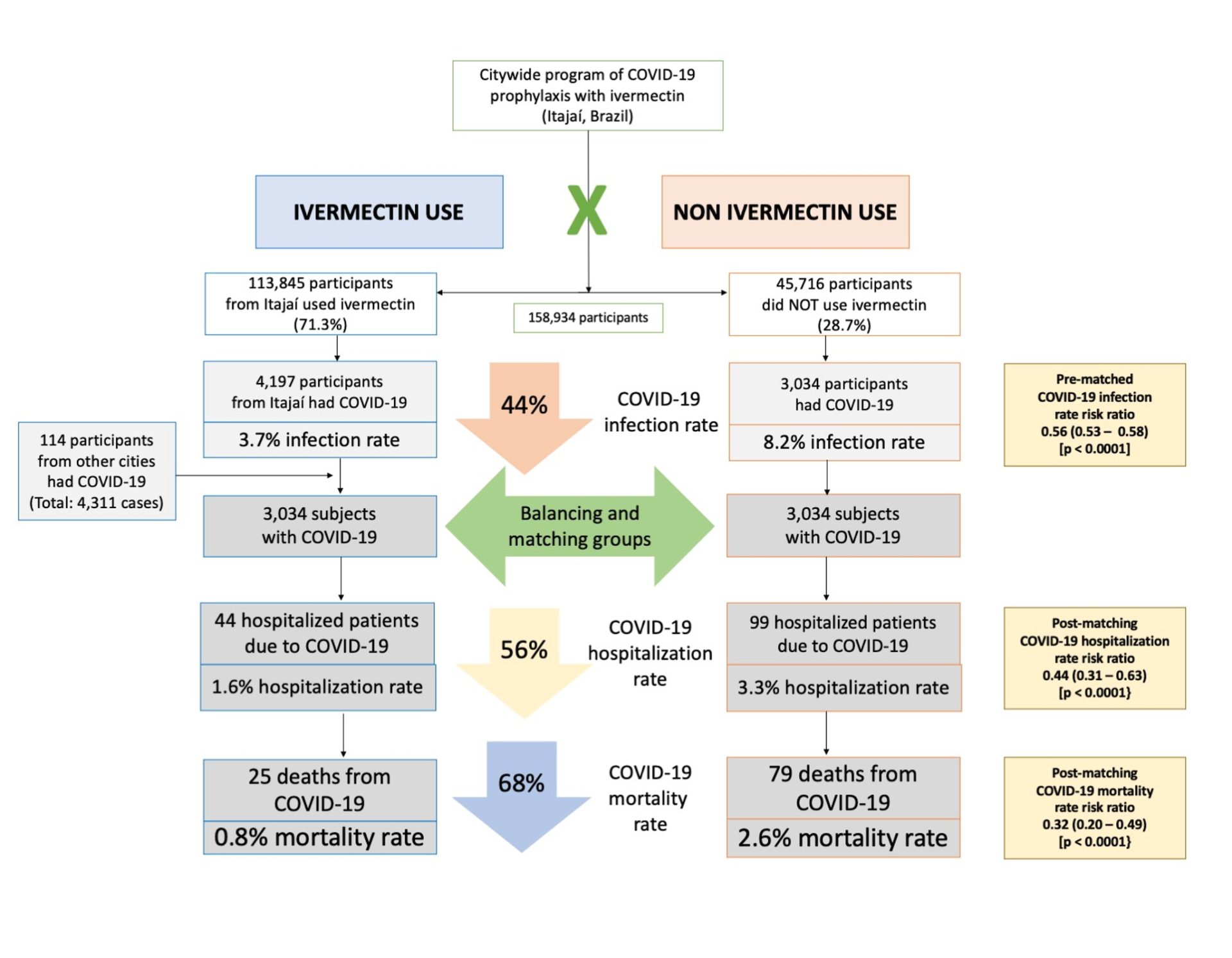
We analyzed data from a prospective, observational study of the citywide COVID-19 prevention with ivermectin program, which was conducted between July 2020 and December 2020 in Itajaí, Brazil. Study design, institutional review board approval, and analysis of registry data occurred after completion of the program. The program consisted of inviting the entire population of Itajaí to a medical visit to enroll in the program and to compile baseline, personal, demographic, and medical information. In the absence of contraindications, ivermectin was offered as an optional treatment to be taken for two consecutive days every 15 days at a dose of 0.2 mg/kg/day. In cases where a participating citizen of Itajaí became ill with COVID-19, they were recommended not to use ivermectin or any other medication in early outpatient treatment. Clinical outcomes of infection, hospitalization, and death were automatically reported and entered into the registry in real time. Study analysis consisted of comparing ivermectin users with non-users using cohorts of infected patients propensity score-matched by age, sex, and comorbidities. COVID-19 infection and mortality rates were analyzed with and without the use of propensity score matching (PSM).
I was confused when I read the paper. Iivermectin was not recommended for anyone to take if they became sick with COVID-19, even though it was offered as a preventative measure.
Patients who presented signs or the diagnosis of COVID-19 before July 7, 2020, were excluded from the sample. Other exclusion criteria were contraindications to ivermectin and subjects below 18 years of age. The dose and frequency of ivermectin treatment was 0.2 mg/kg/day; i.e., giving one 6 mg tablet for every 30 kg for two consecutive days every 15 days.
During the study, subjects who were diagnosed with COVID-19 underwent a specific medical visit to assess COVID-19 clinical manifestations and severity. All subjects were recommended not to use ivermectin, nitazoxanide, hydroxychloroquine, spironolactone, or any other drug claimed to be effective against COVID-19. The city did not provide or support any specific pharmacological outpatient treatment for subjects infected with COVID-19.
This is a rather strange design. When this study began, people were asking the same question as I was: Why on earth would you recommend that patients take two doses, separated by a day, every two weeks?
It's an odd protocol, agreed.
— Kyle Sheldrick (@K_Sheldrick) January 6, 2022
Let's see what the authors claim to have found.
It was summed up thusly.
Of the 223,128 citizens of Itajaí considered for the study, a total of 159,561 subjects were included in the analysis: 113,845 (71.3%) regular ivermectin users and 45,716 (23.3%) non-users. Of these, 4,311 ivermectin users were infected, among which 4,197 were from the city of Itajaí (3.7% infection rate), and 3,034 non-users (from Itajaí) were infected (6.6% infection rate), with a 44% reduction in COVID-19 infection rate (risk ratio [RR], 0.56; 95% confidence interval (95% CI), 0.53-0.58; p < 0.0001). Using PSM, two cohorts of 3,034 subjects suffering from COVID-19 infection were compared. The regular use of ivermectin led to a 68% reduction in COVID-19 mortality (25 [0.8%] versus 79 [2.6%] among ivermectin non-users; RR, 0.32; 95% CI, 0.20-0.49; p < 0.0001). When adjusted for residual variables, reduction in mortality rate was 70% (RR, 0.30; 95% CI, 0.19-0.46; p < 0.0001). There was a 56% reduction in hospitalization rate (44 versus 99 hospitalizations among ivermectin users and non-users, respectively; RR, 0.44; 95% CI, 0.31-0.63; p < 0.0001). After adjustment for residual variables, reduction in hospitalization rate was 67% (RR, 0.33; 95% CI, 023-0.66; p < 0.0001).
The conclusion was leading to it.
In this large PSM study, regular use of ivermectin as a prophylactic agent was associated with significantly reduced COVID-19 infection, hospitalization, and mortality rates.
Everyone should be taking ivermectin two times a week, separated by a day. Should we believe it? Kyle Sheldrake's analysis is one of the reasons not to.
In the paper 6068 participants were propensity score matched from >220,000 patients, 60% of whom took ivermectin.
In the presentation 6068 participants were propensity score matched from 159,000 patients, 77% of whom took ivermectin. pic.twitter.com/ZDpDSbGjIu
— Kyle Sheldrick (@K_Sheldrick) January 6, 2022
And:
And:
In other words, the data is being presented differently. Sheldrake pointed out that the analysis claimed is pretty much impossible and hidden behind the data available upon request.
They've taken those "data available from the corresponding author on reasonable request" statements to the next level.
When are we going to see "title available on reasonable request"?
— longfacehorse (@longfacehorse) January 10, 2022
This study is not a randomized clinical trial, which is how you really determine if a drug treatment works, or if it doesn't, but it has a lot of issues. Some of the issues are similar to randomized trials. It is not clear to me if this is sloppiness or fraud. This is not a good study. It appears to people like Ms. Iverson that it is very impressive. I don't think it was a prospective study. It appears to be a retrospective study.
This was a prospective, observational study. Although study design, institutional review board (IRB) approval, and data analysis occurred after completion of the voluntary prophylaxis program, all data were collected prospectively in real time with mandated reporting to the registry of all events as they occurred during the citywide governmental COVID-19 prevention with ivermectin program, from July 2020 to December 2020, developed in the city of Itajaí, in the state of Santa Catarina, Brazil. Demographic and clinical data were reported from medical records of patients followed in a large outpatient setting (a provisional outpatient clinic set in the Convention Center of Itajaí) and several secondary outpatient settings, as part of the universal health system (Sistema Único de Saúde [SUS]).
Why is this important? In retrospective studies, one looks at the patients in the past. In a prospective study, one sets up and looks at patients as they present and collects the data as it happens. retrospective studies tend to be more bias prone. A prospective data collection for residents of Itajaí is what we appear to have here. If you designed your study after data collection had been completed, you can call it prospective.
Sheldrake described how a huge decrease in mortality could be observed if ivermectin did nothing. He describes it better and more succinctly than I have ever heard before.
The problem with the claim of a "dose-response" relationship in the Itajaí study is that it's a sort of interval variant of immortal time bias.
You would see a massive effect using this analysis even if the drug did nothing.
1/7
— Kyle Sheldrick (@K_Sheldrick) February 7, 2022
No those that died stop taking the bins out when they die.
Does that mean there's a "dose-response" relationship between taking your rubbish out and dying of covid?
It does not.
Something that happens at regular intervals WILL happen less if people die mid way through.
3/7
— Kyle Sheldrick (@K_Sheldrick) February 7, 2022
The authors decided to compare those taking 31+ tablets of ivermectin to those who took none!
Surprise it looks great.
Because ivermectin users who died are almost all removed from the headline analysis.
Controls who die do count though!
5/7
— Kyle Sheldrick (@K_Sheldrick) February 7, 2022
Let's go back to our bins.
If there are 15 bin collection days and we look only at those who have taken yours out 13 or more times, then the death rate (assuming even dist.) will be about… 87% lower than the general population!
Now that's a dose response relationship!
7/7
— Kyle Sheldrick (@K_Sheldrick) February 7, 2022
On to the next study.
Treatment with Ivermectin Is Associated with Decreased Patients in COVID-19 Mortality: Analysis of a National Federated Database is a study. The investigators are plastic surgeons and urologists at the University of Miami. Plastic surgeons and urologists are not the ones who have the right skills to do a study like this. The study is being promoted by FLCCC. Amusingly, one of the authors pushed back.
Hi Dr. Peterson, first author of the paper, I think the information and data is being crudely misrepresented and misinterpreted. This is an abstract (NOT PEER REVIEWED) from a conference I presented at. We did not submit the manuscript for a reason, weak evidence.
— Iakov Efimenko (@AesBrah) March 8, 2022
And he is correct! I didn't notice that it was published in a supplement of the International Journal of Infectious Diseases, dedicated to publishing the abstract from the 8th International Meeting on Emerging Diseases and Surveillance. That's why there is an abstract with no full article. I will give the student credit for being honest. I won't spare his mentors. Students can be forgiven for this bad study if they learn from it.
This is an example of what can happen when you confound by indication. The authors compared patients who received remdesivir for COVID-19 to those who received ivermectin. Can anyone see the problem? The name of the confound should tell you that patients who receive remdesivir are hospitalized, while those who receive ivermectin take it as outpatients. The study didn't correct for the fact that the patients were all hospitalized and that they would do worse.
Or:
World's worst study. Remdesivir has to be used as inpatient therapy so patients are already hospitalized vs an oral drug that you can take at any stage of the disease. Worthless data from the bright minds of the department of Plastic Surgery.
— B&B (@Bladeandbarrel) March 3, 2022
I am less harsh on the students after reading this thread.
New embarrassingly bad study of ivermectin is a textbook example of “confounding by indication”
In short a retroactive database review found that people w/ COVID did worse if given remdesivir (only given to sick inpatients) than ivermectin (only given to well outpatients)

1/ pic.twitter.com/f76tBBmuVl
All Rights Reserved © 2024




