Over the last few weeks, I've noticed a resurgence of messaging that emphasizes natural immunity as being superior to vaccine-generated immunity, particularly for the more recent variant of SARS-CoV-2. Jeffrey Tucker wrote an article on the Brownstone Institute website asking if public health officials have finally admitted natural immunity. They don't want you to know about natural immunity, it's the way out of the epidemic. Fox News and the Wall Street Journal have both had stories about natural immunity, as well as other examples. I want to make my position clear before I get to the science. The use of the word "natural" in the term "natural immunity" has made it very easy to argue against COVID. I have discussed before how scientists made a huge mistake in using the term "natural immunity", because it is an inherently misleading term. Post-infection immunity is the more appropriate term to describe vaccine-induced immunity, with the added advantage of not having to suffer through the disease and risk its potential complications. Natural immunity is often described as having quasi-magical properties, implying that it is lifelong, far better against everything, and even beneficial, with some even going so far to argue that. Even though children do have a lower risk of death from COVID-19, there are still death tolls that rebuke this argument every bit as much as the death toll in the US. It's not just antivaxxers and antimaskers who have started promoting the natural immunity narrative. Doctors who should know better. Activists, pundits, and politicians are co-opting the term "natural immunity" in order to oppose vaccine and COVID-19 mandates. Leaving aside my contention that natural immunity is a horrible term, what is the real situation? It is often complicated with such issues. The science is not consistent with the dominant narrative about natural immunity, so we cannot discuss this question without looking at it. I debated about bringing up the Great Barrington Declaration, having done so just last week in the context of a study that tried to argue that the GBD was overwhelmed. The article is being used to cast opponents as un serious social media creatures. The media narrative on natural immunity and natural herd immunity has been dominated by the GBD, its authors, and its boosters. The ideas behind the GBD were threefold, the first of which was published in October 2020, before safe and effective COVID-19 vaccines were available to the public anywhere except in clinical trials. Proponents of GBD seem to define it as any government public health edict closing businesses or placing restrictions on private individuals. Natural herd immunity is inevitable, and we should adopt a strategy with respect to COVID-19 and healthy. The authors and advocates of GBD have long had preferential access to the media and government. The recent release of a book by Scott Atlas, President Trump's COVID-19 advisor, confirmed this preferential access. The day after the Augusr meeting, the President described his strategy: "sheltering those at highest risk, especially the elderly, while allowing lower risk Americans to safely return to work and to school…they have to get back to work."https://t.co/7sEZgoRzXP pic.twitter.com/zCoI3VgIB0 — Mallory Harris (@malar0ne) February 18, 2022 And it was ≈ a month after HHS Science Adviser Paul Alexander sent an email saying "open up and flood the zone and let the kids and young folk get infected…we want them infected." He now writes for the Brownstone Institute, GBD's "spiritual child."https://t.co/2jdbdhrqmj — Mallory Harris (@malar0ne) February 18, 2022 We also know that the GBD was propped up by right-wing corporate interests, including AIER, the libertarian thinktank that hosted the event where the documented was written.https://t.co/KyHp0C05P7 — Mallory Harris (@malar0ne) February 18, 2022 There were problems with the three ideas behind the GBD. It tended to exaggerate the harms of lockdowns and minimize the ability of them. The assumption was that natural herd immunity was inevitable. To portray COVID-19 as a fatal disease, GBD had to bend over backwards to portray it as amild disease, by lowballing death estimates. Natural herd immunity requires that immunity be long-lived, if not life-long. Natural herd immunity will likely never be reached if immunity wanes too quickly in individuals or virus strains that can evade immunity from previous infections. I can only cite Omicron and the new Omicron subvariant BA.2 as evidence that this has been the case with COVID-19, but even 16 months ago given how the Omicron variant has led to a massive surge in reinfections. Even as long as a year ago, scientists were beginning to fear that herd immunity was out of reach because too high a percentage of the population would need to be immune. The concept of focused protection in the GBD was not defined to the point of being meaningless. It ignored the enormous difficulty of protecting the large segment of the population that is at high risk of severe disease and death, including the elderly and those with chronic health conditions, while a respiratory virus is ripping through the young. It was a profoundly ableist and even the idea that young people should be allowed to be exposed to STDs to protect the vulnerable was a part of the idea. It was a fake proposal, made up by a right wing think tank, which was opposed to the restrictions. It is worth reviewing recent evidence to evaluate the relative value of post-infection immunity because of the political use and misuse of it. It is worth doing so in the context of the Brownstone Institute's founder asking the question about natural immunity. Tucker references a recent CDC study to make his claim.
In late January, the CDC published a report that made what might have been regarded as a shocking claim. If you have had Covid, the CDC demonstrated in a chart, you gain robust immunity that is better than that of vaccination, especially concerning duration. That should be nothing surprising. Brownstone has chronicled 150 studies making that point. What made this new chart different was that it came from the CDC, which has buried the point so deeply for so long as to amount to a near denial. So there: the CDC says it. So nonchalant! So uneventful! If people had understood this two years ago, plus been made more completely aware of the dramatic risk gradient by age and health, lockdowns would have been completely untenable. The society-wide mandates and lockdowns depended on keeping the public ignorant on settled points of cell biology and immunology, plus pressuring social media companies to censor anyone who didn’t fall in line. Here we are all this time later and the truth is coming out. Had the knowledge of risk gradients and immunities been in the forefront of policy makers’ minds – instead of wild fear and obsequious deference to Fauci – we would have focused on protecting the vulnerable and otherwise allowed society to function normally so that the virus would become endemic. We would not only have saved thousands of lives; we could have avoided the vast economic, educational, cultural, and public-health wreckage all around us.
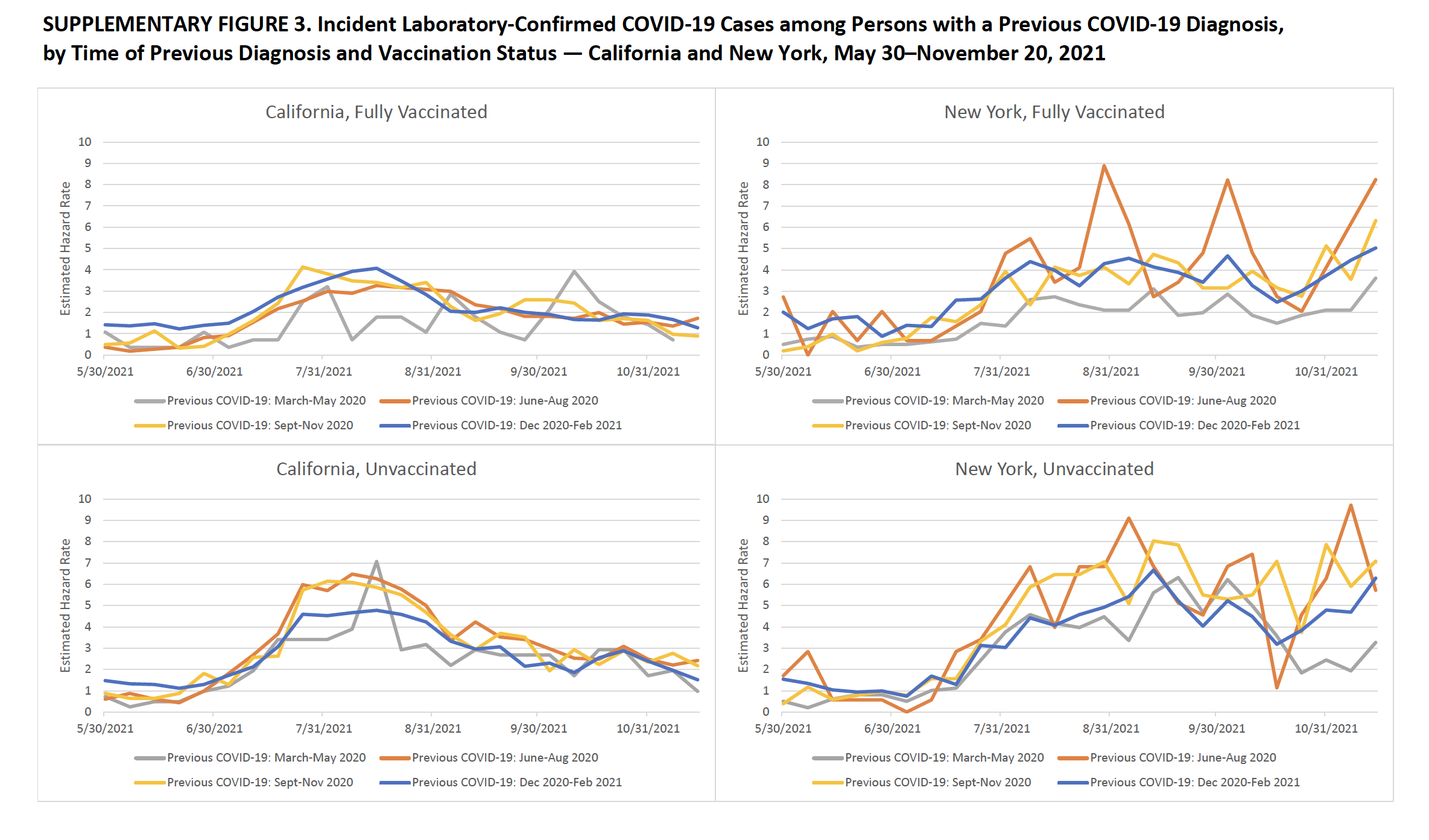
Those poor are advocates for natural herd immunity. Paul Alexander, the HHS science advisor who once wrote in an email that we want them, is a writer for Brownstone. It's a favorite tactic among antivaxxers who don't consider study quality, only quantity. Even though he didn't like what Fauci had to say, he blamed Anthony Fauci. What about that study? The narrative lately seems to be a tale of a couple of recent studies, starting with the CDC study. Tucker was taken by a video analysis written by Dr. Vinay Prasad, who was the author of the study that was published three weeks ago in Morbidity and Mortality Weekly Report. Dr. Prasad was contemptuous of those of us who took the time to refute quackery and antivaccine misinformation even before the Pandemic. He pivoted to becoming a rich source of misinformation, even describing public health interventions as potentially the first step on the road to fascist rule. The entire claim is based on this graph. A lot of work is done in this graph. In order to assess what happened as the Delta wave became predominant, this figure represents data from California and New York, which account for 18% of the U.S. population.
Across the entire study period, persons with vaccine- and infection-derived immunity had much lower rates of hospitalization compared with those in unvaccinated persons. These results suggest that vaccination protects against COVID-19 and related hospitalization and that surviving a previous infection protects against a reinfection. Importantly, infection-derived protection was greater after the highly transmissible Delta variant became predominant, coinciding with early declining of vaccine-induced immunity in many persons (5). Similar data accounting for booster doses and as new variants, including Omicron, circulate will need to be assessed.
We have a snapshot of what happened as the Delta wave revved up but before Omicron crashed onto the scene, which led to different results than what was observed with the original COVID-19 strain, for which vaccine-induced immunity was more potent than post-infection immunity. Is this proof that natural immunity is superior? Not quite. The data doesn't come close to taking into account the effect of the Omicron variant and the increasing number of people receiving boosters. There are at least seven limitations that the CDC noted, among them no stratification of the analysis by time since vaccine receipt, misclassification of people with COVID-19 as having had vaccine, and unmeasured confounders. Another analysis that tries to do that is not nearly as clear. The data doesn't look as clean when presented this way. That's why the CDC concluded.
Vaccination protected against COVID-19 and related hospitalization, and surviving a previous infection protected against a reinfection and related hospitalization during periods of predominantly Alpha and Delta variant transmission, before the emergence of Omicron; evidence suggests decreased protection from both vaccine- and infection-induced immunity against Omicron infections, although additional protection with widespread receipt of booster COVID-19 vaccine doses is expected. Initial infection among unvaccinated persons increases risk for serious illness, hospitalization, long-term sequelae, and death; by November 30, 2021, approximately 130,781 residents of California and New York had died from COVID-19. Thus, vaccination remains the safest and primary strategy to prevent SARS-CoV-2 infections, associated complications, and onward transmission. Primary COVID-19 vaccination, additional doses, and booster doses are recommended by CDC’s Advisory Committee on Immunization Practices to ensure that all eligible persons are up to date with COVID-19 vaccination, which provides the most robust protection against initial infection, severe illness, hospitalization, long-term sequelae, and death.
In this one study looking at the original COVID-19 strain and the Delta variant, post-infection immunity appears to be more robust, but with a lot of caveats. There are a number of other studies and they all say the same thing: post-infection immunity is better than post-vaccine immunity. One study that was published in the Journal of the American Medical Association was trumpeted last month. It was from Dr. Makary's group, which isn't a good sign. Get a load of its recruitment methods.
Healthy adults who reported no SARS-CoV-2 vaccination were recruited via 1 public Twitter post and 1 public Facebook advertisement between September 11, 2021, and October 8, 2021. Participants completed an online questionnaire about demographics, COVID-19 status, and mask use. Using weighted random sampling (relative weights based on the estimated unvaccinated US population by age, race and ethnicity, and education1), we created 3 equally sized sample groups among those who reported a test-confirmed COVID-19 infection (“COVID-confirmed”), believed they had COVID-19 but were never tested (“COVID-unconfirmed”), and did not believe they ever had COVID-19 and never tested positive (“no-COVID”). These groups were invited to undergo antibody testing at LabCorp facilities nationwide.
That is correct, you read that. There was no control group and recruitment was highly dubious. Yet he misrepresented his paper on social media.The Great Barrington Declaration
Did the CDC really say that “natural immunity” to COVID-19 is superior?
The “natural immunity” wars continue
Marty Makary, MD, MPH, February 3, 2022.
I'm going to quote Dr. Makary and his colleagues in the Discussion section.
Study limitations include lack of direct neutralization assays, the fact that antibody levels alone do not directly equate to immunity,4,6 the cross-sectional study design, a convenience sample with an unknown degree of selection bias due to public recruitment, self-reported COVID-19 test results, the study population being largely White and healthy, and lack of information on breakthrough infections. Participants were given only 1 month to complete antibody testing, which may have contributed to the 52% rate among those invited to test.
I think this takedown is entirely justified.
The New England Journal of Medicine published a study that showed that previous infections were not as protective against the Alpha variant as they were against theBeta variant. A previous variant of Omicron is only protective against infections with a previous variant.
There is a recent Nature paper that used both functional neutralization and antibody quantification for the purpose of determining the presence of the SARS-CoV-2 spike protein binding domain on cells in order to facilitate the entry of the virus into the cell. To cook it down.
In this study, we showed that mRNA vaccinated blood donors have a median of 17 times higher RBD antibody levels when compared with those who became seropositive due to prior COVID-19. Our results indicated an exceptional strong association between high RBD antibody levels in and the ability to biochemically neutralize RBD binding to the cellular ACE2 receptor. The N501Y mutation, while did not alter the neutralizing antibody binding, presented with a fivefold greater affinity to ACE2, which resulted in a drastically reduced ability of COVID-19 convalescent antisera to neutralize its ACE2 binding. Fortunately, the vaccinated blood samples, due to their much-elevated RBD antibody levels, were far more effective in neutralizing both the WT and N501Y RBD from binding to ACE. With an average of 16-fold greater potency than convalescent blood, the vaccinated blood samples were more than sufficient to compensate for the fivefold increased affinity of N501Y RBD, resulting in the highly effective inhibition of both the WT and N501Y RBD from binding to ACE2.
The last part is important. The Omicron's immune escape doesn't result in a decrease in binding to theRBD, but it does result in a decrease in binding to theACE2 receptor. Only 33 donors with previous COVID-19 and 38 samples obtained from the Department of Laboratory Medicine ofNIH are included in the preliminary study. The study suggests that the levels of the immune system are waning after 6 months.
From my perspective, it appears that the vaccine is just as effective as the infection-inducing one, but not as effective against later versions. Regardless of whether one views this natural immunity as superior or more robust than immunity from the vaccines, the term "natural immunity" will always be used. Even if post-infection immunity were to be found to persist two or three times longer than post-vaccination immunity, it would still not be enough to end the epidemic.
It is simplistic to look only at the natural immunity dichotomy andvaccine-generated immunity. How do we maximize protection against COVID-19, regardless of prior infections and variant?
There are studies looking at hybrid immunity, or immunity to COVID-19 produced as a result of the combination of infections and vaccinations. There is another term being used for this type of immunity.
Another study, conducted by Oregon Health & Science University, found that a breakthrough infection in a vaccinated person leads to “super immunity.” The study compared blood samples from 52 Pfizer-vaccinated employees of the university infected with different strains of the virus—Alpha, Beta, Gamma, and Delta.
The study found that antibodies measured after breakthrough cases were more abundant and more effective than antibodies generated two weeks after a second dose of the Pfizer vaccine. “You can’t get a better immune response than this,” said Fikadu Tafesse, the author of the report and an assistant professor at the OHSU School of Medicine.
Readers could easily have predicted that I would dislike the term "super immunity" more than I dislike the term "natural immunity". It's possible that I missed a study, but let's look at a quick rundown of what I found.
A recent Israeli study published in Annals of Internal Medicine compared the incidence rate of re-infection of people who had previously received a single dose of the Pfizer-BioNTech vaccine with people who had not. The data used in this study was mostly from before the rise of the Omicron variant. Nonetheless:
A statistically significant decreased risk (hazard ratio, 0.18 [95% CI, 0.15 to 0.20]) for reinfection was found among persons who were previously infected and then vaccinated versus those who were previously infected but remained unvaccinated. In addition, there was a decreased risk for symptomatic disease (hazard ratio, 0.24 [CI, 0.20 to 0.29]) among previously infected and vaccinated persons compared with those who were not vaccinated after infection. No COVID-19–related mortality cases were found.
There was no statistically significant difference in the number of hospitalized patients. That's why a doctor who we have met before and who should know better is claiming that the study doesn't show any benefit from vaccination after an infection. The point is that the numbers of hospitalized patients were too small to determine if there was a statistically significant difference between the two groups.
There were two studies published in last week's NEJM addressing this question, one from the SIREN study group and the other from the Israeli group. The SIREN study is a multicenter study involving health care workers in the United Kingdom and consists of people who have not been exposed to the disease but have been tested for it every 2 weeks. Clalit Health Services maintains two databases for the Israeli study. Both suggest that hybrid immunity is better than either vaccine orinfection.
The SIREN study began in June 2020 and included 35,768 participants, of which 27% had a previous SARS-CoV-2 infection. Because of the prospective nature of the study, it was possible to follow the participants over time and determine their risk of getting infections. The Pfizer/BioNTech vaccine provided excellent short term immunity, but it waned after 6 months and the immunity from prior infections waned after a year. After a year, the best immunity came from a combination of prior infections and vaccinations.
The second study found that the cumulative risk of reinfection was lower in people over the age of 65 who had been vaccined. Those who remained unvaccinated were four times more likely to be re-infected.
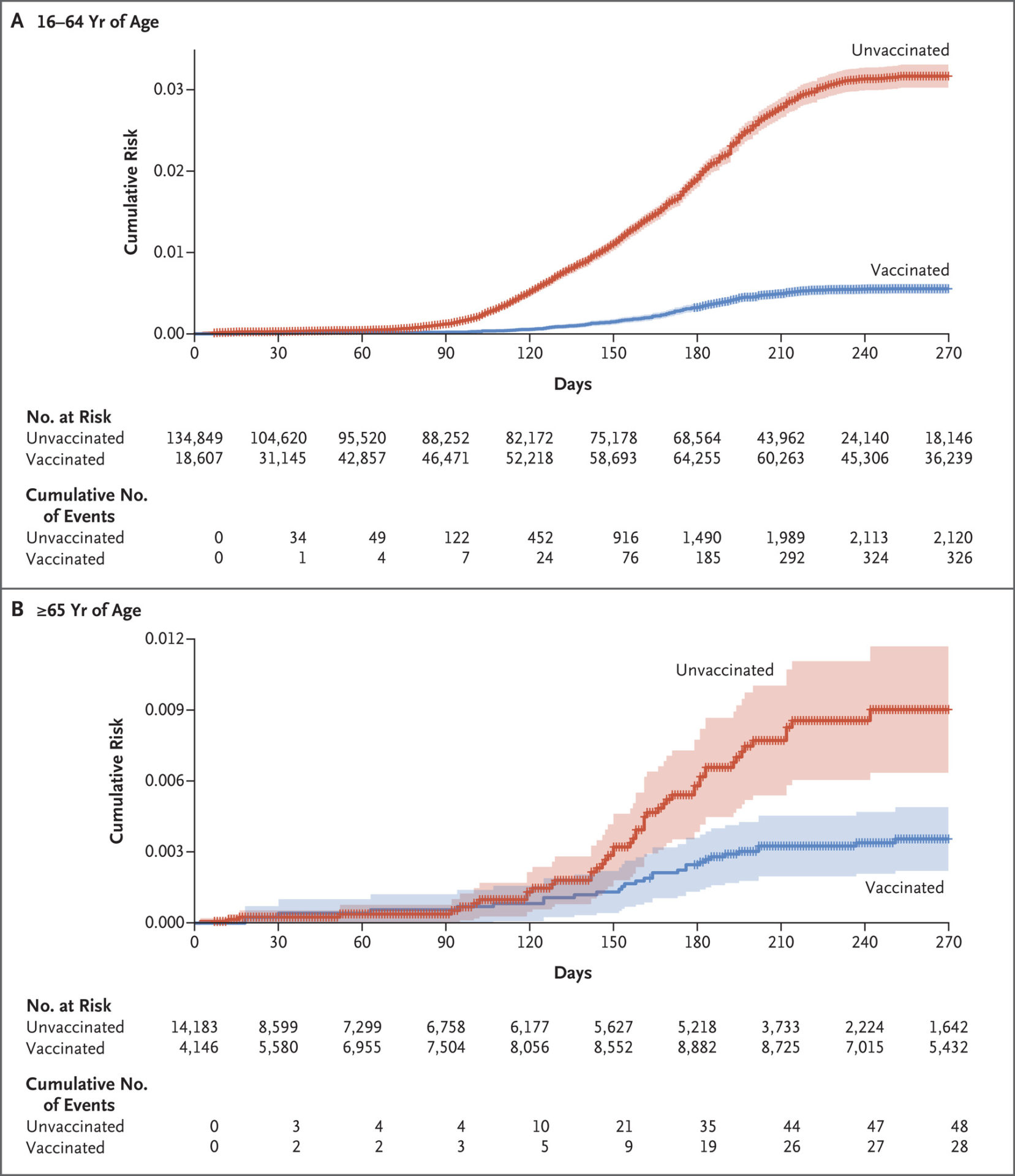
There was no difference in vaccine effectiveness between those who received one dose or two doses after infection and those who did not, in line with other studies suggesting that one dose is sufficient in people who recovered from COVID-19.
The concept of hybrid immunity is supported by laboratory studies. Steve Novella wrote about one of them last month, but I won't retread the same ground, other than to say that human immune sera following a breakthrough infection and vaccination following natural infection can broadly neutralize the virus.
A recent study out of OHSU suggests that breakthrough infections work the same way, boosting humoral immunity after vaccination with the Pfizer/BioNTech vaccine. A preprint from a different group suggests the same thing. The studies only had 52 participants in the first study and only 23 in the second study, but they did measure the neutralization of the virus by the immune system. I'll wait until the second paper is published in a peer-reviewed journal to be surprised if larger studies confirm these observations.
Why does hybrid immunity seem to be more effective against the disease? One of the investigators of the study said that.
According to Crotty, hybrid immunity allows the body to create more diverse antibodies to neutralize a wider variety of variants. This also happens with full vaccination and a booster, but it happens much faster with infection followed by vaccination.
“Hybrid immunity has got a whole bunch of additional bonuses to it. One, that these studies are showing quite presently, is durability. Durability is quite robust,” Crotty said.
This makes sense, of course, although I always remind people that science does not mean that it will be true. I don't like the idea that the Omicron variant could be Mother Nature's way because of the study that found enhanced immunity to other variant after breakthrough Omicron infections.
I asked if natural immunity was better than vaccine immunity. There are differences between them. Think of it this way. It is better not to get COVID-19 because of the risk of death and cardiovascular problems. Vaccination is preferable because it confers immunity without the potential risks. There is nothing magical about natural herd immunity, contrary to the narrative promoted by advocates. It probably lasts longer, but it's not as long as people say it is, and it's not as long as new versions of it. If you have been unable to avoid getting COVID-19 and are fortunate enough to have recovered, it is a good idea to get a vaccine.
No one in public health is against natural immunity and no one is against vaccine mandates. I'm going to quote this because it's a massive straw man.
We know how the immune system works. We know that you’ll probably produce some antibodies and will likely have some T cell memory after an infection. BUT. We also know that this response is variable. We don’t know how long your antibodies will last.
— Leah B. Gilliam, MD (@DrGRuralMD) November 14, 2021
There may be some difference in immune memory between those with mild infections and those who have been more seriously ill.
— Leah B. Gilliam, MD (@DrGRuralMD) November 14, 2021
We recognize it. But we also acknowledge the reality that it’s not absolute – and we’re ok with that because NOTHING in medicine is absolute. It makes sense that this wouldn’t be either.
— Leah B. Gilliam, MD (@DrGRuralMD) November 14, 2021
So please, if you’re reading this and you want to argue with a healthcare worker about whether or not these vaccines are necessary, come up with a better argument than “you need to recognize natural immunity!”
— Leah B. Gilliam, MD (@DrGRuralMD) November 14, 2021
I would counter that the people who tout post-infection natural immunity and natural herd immunity are the ones who are actually superior to vaccine-generated immunity. The ideologues behind the efforts of the GBD exaggerate their preferred solution and contort their science to justify it as vaccine free. We are not opposed to that if it involves treating a prior COVID-19 infection like one course of vaccination. Good evidence that this is a sound strategy is what we want. The idea that lockdowns do more damage than COVID-19 and that mask and vaccine mandates are unacceptable assaults on individual freedom is the start of the argument by the proponents of GBD. Ask yourself why the anti-lockdowners and antimaskers have aligned themselves with the antivaccine movement, given that there is no more powerful tool than the vaccines to implement an actual policy.
Medicine and its related specialty public health can never be purely science, so we call it science-based medicine. Science can give us parameters of what we can do by giving us interventions to combat the pandemic, but in the end value judgments over the tradeoffs involved are based on a given society's values. The values of the GBD are clear, and they don't mean the minimization of suffering and death. They have wielded outsized influence compared to their numbers.

You can buy an e-book.
Dr. Hall has a video course.
The text is powered by the internet.
Powered by TranslatePowered by Translate
TranslatePowered by Translate
All Rights Reserved © 2024




