Thank you Mr. Allely.
I just read your article about myocarditis in young boys. You wrote about yourself, a healthy 25-year-old male, and said, "I faced a far higher risk of being hospitalized with the vaccines I was mandated to take than if I had simply been infections with Covid." You said that the data shows that we may have inflicted a greater number of hospitalizations on young boys by vaccine.
I was expecting more from the student. How you came to your conclusions, why they were flawed, and why I think the doctors in charge of Sensible Medicine owe you an apology are some of the topics we are going to discuss.
There is a risk of myocarditis from the vaccine in males from 16 to 29 years of age. It's about 1 in 10,000. The rate of vaccine-myocarditis varies from one study to the next, but it seems reasonable to me. The only sensible part was this one.
You criticized Dr. Eric Topol for describing vaccine-myocarditis as "mild".
Whether a median of three days of hospitalization can ever be considered mild is another question. I would argue that if you take a healthy young middle school boy and put him in the hospital for a few days you’d damn well better be sure the upside from your intervention is far greater.
You didn't tell your readers that vaccine-myocarditis is not just Dr. Topol. You cited a paper from Israel.
The clinical course appears to be mild and benign over a follow-up period of 6 months, and cardiac imaging findings suggest a favorable long-term prognosis.
There have been grave outcomes, including the deaths of a few young men, but they are vanishingly rare. None of the papers you quoted were in this collection.
You say vaccine-myocarditis shouldn't be called "mild". When a child is hospitalized, we both agree that it is a big deal. Your argument about calling vaccine-myocarditismild isn't just with Dr. Topol, it's with dozens of doctors from around the world who wrote the papers we read and cite. Readers won't know what you're saying. They will think it was just Dr. Topol.
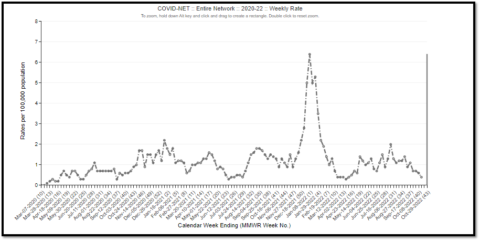
It was clear that your discussion of COVID's risk was incorrect. I don't know what to say about it. You mentioned the CDC MMWR titled Hospitalization of Adolescents Aged 12–17 Years with Laboratory-Confirmed COVID-19 - COVID-NET, 14 States, March 1, 2020–April 24, 2021. It was discovered.
COVID-19 adolescent hospitalization rates from COVID-NET peaked at 2.1 per 100,000 in early January 2021, declined to 0.6 in mid-March, and rose to 1.3 in April. Among hospitalized adolescents, nearly one third required intensive care unit admission, and 5% required invasive mechanical ventilation; no associated deaths occurred.
The data is the worst case scenario because no adolescents werevaccinated at this time. You said something.
At the peak of hospitalization from Covid in this age group, 2.1 per 100,000 adolescents were hospitalized with Covid. None died. Pfizer’s vaccine data from the NEJM study suggests that just under 9 per 100,000 adolescent boys were hospitalized with myocarditis. None died. So risk of hospitalization from Pfizer’s vaccine series may have been over four times as likely to land a young boy in the hospital than Covid over this time period.
This is not right. One at a time, let's go over the issues. You stated that no adolescents died, which was correct for 204 hospitalized adolescents. The data isn't telling the whole story. About 10% of the US population is covered by the Covid-NET. It's important that the other 90% is also important. The data from 43 states was collected by the American Academy of pediatrics. Some adolescents died of carbon dioxide. Readers who are incorrect won't know this.
Your comparison is completely ridiculous. The risk of an adolescent being hospitalized was 2.1 per 100,000 the week of January 9th, 2021. They weren't at risk of being hospitalized during the first 13 months of the Pandemic. It would have been correct to say that the risk of hospitalization from Pfizer's vaccine series may have been over four times as likely to land a young boy in the hospital than Covid. Every vaccine would fail if it were judged this way.
The hospitalization rate for adolescents should have been higher than 2.1 per 100,000. Thousands of adolescents have been hospitalized
You didn't give a reason for why you decided to only look at the risk of the virus from March 1, 2020 to April 24, 2021. I wonder if COVID vanished after this. It is not possible to say yes. The second year of the Pandemic was worse for children. The Delta and Omicron variant caused a lot of illness in children. The time period from March 1, 2020 to April 24, 2021. The Omicron wave was responsible for 20% of the deaths of children. In the month of January, about 180 children died from carbon dioxide. Readers who are incorrect won't know this.
The hospitalization rates are for 12 to 17 year olds.
To your credit, you acknowledged that vaccines decrease the risk of severe disease, and that the Delta and Omicron variant would have taken a much greater toll on adolescents if they hadn't beenvaccinated. The vaccine-advocates have always said this. It is an important point and you changed your readers by ignoring it.
The CDC MMWR titled Characteristics and Clinical Outcomes of Children and Adolescents Aged found that there was one vaccine-eligible patient who was fully vaccine free. I think that is a pretty big deal. Why didn't you mention this to your readers?
Some children who were hospitalized with COVID died. The report said that.
Approximately one half (54.0%) of patients hospitalized for COVID-19 received oxygen support, 29.5% were admitted to the intensive care unit (ICU), and 1.5% died; of those requiring respiratory support, 14.5% required invasive mechanical ventilation (IMV).
Neurological problems are not uncommon in children hospitalized with Covid. It is rare and mild if we want to use Dr. Topol's standards.
Is that really true?
There is a difference between a child hospitalized for a few days with vaccine-myocarditis and a child intubated for over a week with Covid.
My message, technically is: If you’re eligible to get the vaccine, please do. I plan on getting vaccinated as soon as my doctor lets us know when I can.
She had to relearn basic motor skills while in the hospital. It is not uncommon for such outcomes with COVID. Children have had amputations or strokes. healthy teenage boys who were eligible to be vaccine free have died of Covid Most of the children who suffer from MIS-C go to the intensive care unit. There have been 74 deaths of children. The grave outcomes from vaccine-myocarditis are very rare. There are no known deaths from it.
Readers won't know anything about this. The vaccine has already protected many children from the worst harms of the virus, and you didn't mention it. According to studies, only unvaccinated children died of Covid.
I don't think I'm a mind- reader. I don't know if the glaring omissions and inappropriate comparisons were because you didn't know basic information or if you deliberately neglected to mention anything that would undermine your argument. The good news is that there is a simple way to prevent this from happening in the future. Ask someone who is an expert to read your article before you write it. They will give you a perspective you don't have.
I'm sure there are doctors at your medical school who can give you an idea of what it's like to care for a sick kid. Talking them would be more useful than having a conversation with the doctors at Sensible Medicine. You might be able to ask them if their hospitals were filled with children suffering from vaccine side-effects. I believe I will know what they will say.
Other experts will help you as well. Dr. Frank Han has published on vaccine-myocarditis and has treated children during the swine flu. I think he would be interested in reading your article. I have asked for his help before, because I am not an expert in children's cardiovascular disease.
I'm concerned that there may be a bigger problem. I don't think you were careless. I am concerned that you presented only the information that would advance your narrative. I worry that you didn't share facts that would have a positive or negative effect on the vaccine.
Writers on Sensible Medicine tend to have this trait. If ten data points are needed to understand the risks and benefits of the vaccine, they cherry pick the three that support their position. When children get sick, some doctors at Sensible Medicine want unvaccinated children to get COVID. RFK Jr. is one of the leading anti-vaxxers.
I can't help doctors who don't care about accuracy or thoroughness. I can let you know. I recommend that you read a previous article about the dangers of doctors saying outrageous things to make themselves look better. Having the wrong audience is worse than having no audience according to an article.
I think my article will make you angry. You will feel like a victim. Everyone feels that way. There is a temptation to dismiss what I have said simply because it was critical. I have had to make some changes to my writing here. The people pointed out my mistakes. People who disagree with us can point out our flaws. It is guaranteed that you will not improve if you surround yourself in an echo chamber.
The editors of Sensible Medicine did you a disservice by allowing you to publish your article. They owe you an apology and that's very serious. It was their job to help you understand your limitations and make sure your writing was good. They didn't succeed you. They're safe in their careers. It's just beginning.
I want to help you in ways they won't.
The people who oppose child COVID vaccines are conflicting with the experts. The people who cared for sick children during the Pandemic were these. They might be incorrect. Even a medical student can challenge them. You have to back up your argument with thorough, rigorous data, not just the data points that fit your narrative. If you expose a 14-year-old football player to a virus that could kill him, you need to make sure you have a reason not to vaccine him.
David Brin said that it was fun to pretend that you are smarter than doctors with real-world experience and responsibility.
All Rights Reserved © 2024




