The Department of Clinical Tropical Medicine published a preprint on COVID vaccination-associated myocarditis, one of the only potential analyses of asymptomatic COVID. While it is a strong effort from a team who had very little time to put together the project, there are multiple actors who distort the cardiac evaluation that was done, which requires immediate discussion from a board-certified physician.
While not being completely solved from a mechanistic standpoint, COVID vaccination myocarditis is a well-known disease process that is associated with the same type of COVID vaccinations. Older boys and young adults are at risk. National health agencies like the Canadian NACI and the US CDC are trying to find ways to decrease the risk of vaccine-associated myocarditis after the 2nd dose. Transient autoimmune reactions that fall within the realm of hypothesized mechanisms include a reaction against a lipid nanoparticle, a reaction against a distant target, and a potential immunity reaction. The aim of the present study was to determine the incidence of myocarditis in a group of students after they received the second dose of COVID vaccine.
Two-thirds of the 301 students analyzed were boys. They tried to record baseline characteristics of these children. Not all of the data at each of the points was displayed in the preprint version of paper as the team tried to repeat that assessment.
According to the data displayed to the reader, some of the kids met criteria for myocarditis, which included EKG changes, troponin in the blood, and cardiac magnetic resonance findings. Subclinical myocarditis and abnormal EKG findings are reported by their students. The diagnosis of myocarditis is supported by the MRI findings, but the rest of the patients' EKG findings need to be discussed because characters who want to maximize fear surrounding myocarditis are hyping the findings. The crowd thinks that abnormal EKGs alone are enough to diagnose subclinical myocarditis, which is wrong. The least one can do is compare the findings before and after. The EKG findings are not available to the reader. It is difficult to compare the rates given in this article with the rates used in the prior population studies due to their different statistical methods. The troponin elevation may be due to the amount of time it takes for the immune response to kick in. What has been discovered in prior projects on vaccination myocarditis is mirrored by the timing of troponin elevation. troponins are useful for confirmation of myocarditis, but it is not the only cause of troponin in the bloodstream.
The paper discusses the EKG findings.
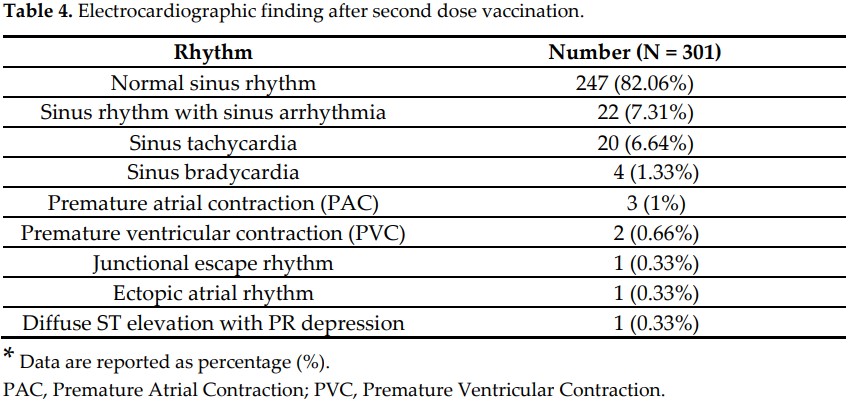
Bad actors may say that 18% of the EKGs were abnormal, but this number is derived from simple subtraction without acknowledging which of these EKG findings are normal variants. They are trying to use these findings to convince people that all the EKG findings demonstrated are abnormal, which, as any medical student or trainee physician should know, is patently false. Some people will use the argument at this point that “no science is settled”, but this knowledge is one of the foundations of general pediatric cardiology. These fundamental EKGs have extremely precise definitions that have no room for debate. I will refrain from using technical terminology as much as possible in the next paragraph, where I will define these different EKG results and what they mean.
All Rights Reserved © 2024




